Correct.
Didn’t get obvious symptoms in my good ear until perhaps 12 months after the injury.
How are you doing at the moment? How long ago was your incident?
Correct.
Didn’t get obvious symptoms in my good ear until perhaps 12 months after the injury.
How are you doing at the moment? How long ago was your incident?
Have you had an audiogram done? It tests pressure in your ear to detect fluid. I was misdiagnosed for 6 years with eustachian tube dysfunction and fluid in my middle ear, but in reality it was vestibular migraine causing my symptoms. Ear fullness can be a migraine symptom. Doctors can’t see fluid in your ear unless your eardrum is bulged outward, and often diagnose ear fullness as fluid because they are unaware of other causes. You may have fluid trapped but i just wanted to tell you my experience to make sure you haven’t been misdiagnosed. I was given steroid nasal sprays which only worsened my symptoms because they trigger migraines. So do be watchful.
‘Vestibular migraine’ is not an aetiology, its a class of condition, defined by a set of symptoms (so might be several things/different root causes with the same constellation of symptoms) Migraine can’t explain fluid in your middle ear, its a neurological disorder. Let’s not lose a sense of reality here!
I’ve woken up every day for 3.5 years with some level of fluid in my middle ear and sometimes it squishes in my eustachian tube (easy to prove, I can massage it through my neck).
I only started having migraines a year into that. For a glorious 6 months I was otherwise completely symptom free. It is not migraine. Anyone who has told you that is going well beyond what science has so far established… That kind of BS makes me very angry and gives the discipline a bad name.
Agree it might not be ETD (I understand you can test for ETD with a simple test of ear drum response to pressure) … I suspect it’s an artefact of PLF or if chronic more likely Secondary Hydrops (which can be brought on by an injury that may or may not have involved PLF). Secondary Hydrops has the same symptoms and treatment as MAV (including the diet!) Go figure!
In short: You may well have a reasonable diagnosis of vestibular migraine (I have had a MAV diagnosis as well as, separately, diagnoses of Secondary Hydrops), but that doesn’t explain the fluid in your ear in so far as it doesn’t explain the root cause. No-one in science has determined a root cause. That’s the rub. In my case I was (un)lucky to have an ear injury immediately prior to my dizziness, so the culprit is very obvious & straightforward (but something a highly paid neuro-oto initially ignored because of the crazy reality distortion field that so blights this area of medicine). As far as I can judge the only reason I’ve not been labeled with MAV by all doctors is because I have clear evidence of trauma.
I love that my little ole “Fluid in eustacian (sic) tube” thread has been so fruitful a discussion!
So I consulted doctor Google after starting this conversation and began holding my nose and blowing out my ears a few times a day, and that seemed to clear up my symptoms. (Don’t try this at home kids without your doctor’s permission!) I had been hiking the PCT and flying a lot this summer so the elevation was affecting me. I seem to be done with those symptoms (fluid in ear feeling) but the ENT warned they may come back. She recommended taking Afrin on flights, which I did not do over the last few days (flying 4 times in 5 days.)
I agree with James here - you can’t always have a confirmed diagnosis; I certainly don’t. I have been told: secondary hydrops, MAV, MdDS and my all-time favorite, “vestibular idiopathy with unknown etiology.” That last is the most accurate ![]()
Agree that if you are suffering from this crp you need to make sure your tubes are clear for flights or you are inviting trouble. In the UK we have sudafed. A good yawn and a neck massage might help too though ![]()
How long did you tubes seemed blocked for? I was diagnosed with ETD aswell, haven’t had a days rest in nearly four months with it to some extent or the other… defo related to my VM diagnosis though as comes on more if I eat, smoke or drink alcohol etc. Any tips how to get rid as I’ve tried lots including nasal sprays also from docs x
I was misdiagnosed with fluid in my eustachian tubes for 6 years. It was actually vestibular migraine. The feeling of fluid, or fullness, or pressure in the ears is a vestibular migraine symptom, caused by either swollen blood vessels, or nerve sensations (so goes the theory). You can feel that fluid is trapped there, and can even hear crackling, but there is so fluid. The only way to know fluid for sure is an audiogram, which tests ear pressure. I had one done and it was normal so the ENT said there is no fluid. It’s a migraine symptom. I was given a steroid nasal spray by my GP, which only increased the severity ofmy symptoms, which makes total sense because blood vessel dilaters trigger migraines. If you are on any decongestants, stop taking them. Get an audiogram done if you haven’t already to test for fluid. A doctor cannot diagnose fluid by looking in your ear, they cannot see it, they just assume all ear fullness is caused by fluid. I can’t believe my vestibular migraine was misdiagnosed for 6 years as being eustachian tube dysfunction, but apparently its quite a common misdiagnosis.
It’s fluid. Let’s not let some doctors create a ridiculous reality distortion field. I can actually squish that fluid in my tube by massaging the back of my neck. I’ve heard it glugging, bubbling, popping. It’s definitely fluid! Sometimes it dulls your hearing, even can make you hear your own voice, then you can feel it leak away and your hearing returns to normal.
And I doubt its related to nerves or blood, it’s probably perilymph released from the inner ear.
And btw, they’ve found a pressure release valve in the inner ear this year - imagine - a major part of the inner ear ONLY DISCOVERED in 2018! Gives you a clue to the state of the discipline!
https://www.mvertigo.org/t/inner-ear-pressure-release-valve-found/15685?u=turnitaround
On top of this it could well be a spontaneous PLF to dump pressure (though this is contentious).
This is the reason people don’t get glaucoma of the ear - it has an ability to release over-pressure and this protects the inner ear structures and its neurons - and your balance & hearing!
And doesn’t it strike you as more than co-incidence that the eustachian tube passes into your throat and as such carries away any additional fluid harmlessly? It’s almost as if this has evolved to happen?!
Furthermore they’ve started finding evidence of Hydrops (inner ear pressure) in patients initially diagnosed with VM. That’s because scanner techonology has finally got to level it needs to get to identify Hydrops on MRI in the clinic. We’re about to see a big change in diagnosis I suspect and possibly a major change in the hypotheses. I’m sure this will lead to further insights, better focus and new solutions.
NB If reading medical journals makes you anxious, don’t do it
Fair enough, but i would still want tests to confirm actual fluid, because then you can work on getting the right treatment or looking at causes of why the fluid is trapped, or if you have an allergy or physical problem. I had an mri of the ears which found everything normal, so i know there is no fluid in my case and the vm diagnosis is correct. If you haven’t had any scans or an audiogram then i’d definitely get them done.
And that’s a can of worms.
There is no current clinical protocol in the West to collect or test this fluid (presumably because of a mainly conservative approach - they’d have to open up your ear drum to get to it).
Studies have happened in Japan in relation to PLF to identify perilymph in the middle ear space.
e.g https://www.tandfonline.com/doi/abs/10.3109/00016480903508910?journalCode=ioto20
Shocking really given how common this symptom is.
Most clinical MRI cannot resolve the inner ear - have you looked at yours in detail? Can you see the Reissner membrane? MRI, as I understand it, is currently used to rule out neuroma’s and look for signs of MS? The commonly available ones in the clinic are not at all a good tool to look at the inner ear.
This is where the big leap is going to happen.
Most clinical MRI is max 1 or 2T. The new ones are 3T and combined with other improvements they can start to resolve parts of the inner ear.
Most images of the inner ear we see in journals come from sacrificed animals (sadly).
the “VM” diagnosis is presumably correct but purely on meeting committee criteria. It doesn’t actually explain your symptoms, just agrees you have a set of them that match the criteria. That’s how you get such a diagnosis. It explains zilch!
Thank-you for saying that. It drives me bonkers that ENT doctors simply look into the ear canal at the eardrum, and then say, “I don’t see any fluid level”. If you have perilymph and CSF draining down, it’ll exit through the Eustachian tube, down the back of the throat. It drives me even more bonkers when they say, “You just think you feel fluid.”
I emailed the acting director of the National Institutes of Health’s National Institute on Deafness and Other Communication Disorders (NIDCD), because in 1990, the same organization put out a Request For Applications to develop a biomarker to detect leaking perilymph. File attached here here (199.6 KB). She put me in touch with the Director of Central Pathways for Hearing & Balance Program, who then provided me with the contact info for the Clinical Trials NIDCD Program Officer.
I was on the phone with them yesterday, and explained that Japan is ahead of the US with respect to their research on diagnosing PLF. I was given information about the 1990 RFA. What came of it was a 5 year grant made out Steven Telian. The grant number is 1-U01-DC-001285-01 and is entitled “DEVELOPMENT OF CLINICAL MARKER FOR PERILYMPH FISTULA”. It was for a 5 year study, and the amount of money awarded was $897,500.
It seems like it didn’t go much further than that, however. Ikezono et al. have been doing their own thing with Cochlin-tomoprotein, and they’ve been objectively diagnosing PLF with myringotomy and middle ear lavage with saline.
I think it makes tremendous sense to get in touch with the powers that be at Johnson & Johnson, as they own Acclarent, which is the manufacturer of the Acclarent Aera: https://www.acclarent.com/solutions/products/eustachian-tube/aera
Given that many clinics now have this, and given the anatomy it addresses, it makes sense to piggyback on the already-existing tools and methods out there. What needs to be designed and deployed is an absorptive attachment/tamponade-like sponge thing that would get inserted into the lumen of the Aera instead of the balloon. This is a tremendously important accessory that would then get inserted into the lumen of the cartilaginous Eustachian tube to capture any and all fluid egress before it oozes its way down into the back of the throat.
I’d have guessed that this sort of thing already existed, but it seems that it doesn’t. Time to progress!
Dr. Hain made an astute observation that doctors who believe that PLF “don’t exist” are behaving like the “see no evil” monkey (with its hands over its eyes). It’s textbook Semmelweis reflex, explained really well in this article: The Dirty History of Doctors’ Hands | Method
It’s up to us to turnitaround.
There are additional aspects to consider though. I’ll write more tomorrow … :).
Yes.
I’m inclined to think some are either lazy or it’s a bare-faced lie (they don’t want you to know that they don’t know!)
Part of the issue is some are very condescending towards their patients who actually know a lot more about the symptoms than they do!
There is another possibility: that some doctors are trying to spare the sufferer some anxiety. I think this backfires in many cases though because many patients simply want to know what’s wrong with them and why!
The patient is then left with incomplete answers and uncertainty and that ensures many continue to seek answers and spend yet more money on specialists that they might have avoided spending.
(I personally ended up seeing 4 consultants!)
How much?! It didn’t go far with that amount of money? Crazy! Did they publish anything?
I’m with you 100%.
I was particularly taken with your article and this statement:
“the kneejerk reflex to reject new evidence contradicting established norms.”
As I’ve written elsewhere, I believe Migraine Associated Vertigo is a disease involving the inner ear not just the brain and the dogma and simplistic focus on the neurological symptoms seems breathtakingly shortsighted and unhelpful to the long-term development of treatment for this condition.
You can even see neurologists, desperate to defend their previously published work on the matter have the audacity to suggest the ear is having a stroke as a result of the migraines and this explains inner ear symptoms, instead of admitting that the overwhelming number of patients with ear symptoms suggests that the issue is probably down to an instability in the inner ear and loss of homeostasis (and as a result neurological fallout).
Do you have an illustration of this?
Developing a conservative test for perilymph that could be deployed not just for diagnosis of suspected PLF patients but all patients with chronic dizziness reporting symptoms of fluid sensations could definitely finally throw this ridiculous state of affairs into the bin of history.
One thing to note though: this is the tip of the iceberg. We really need much more research into homeostasis of the inner ear. PLF often results in Hydrops (we don’t know how much because there is neither a clinical test for PLF nor an official measure of Hydrops - though an MRI test is starting to be adopted at a clinical level, finally).
Thanks a lot for sharing your research, Thomas. Very happy to provide a place to voice any more insights around this.
https://www.youtube.com/watch?v=hJMort6YCI4
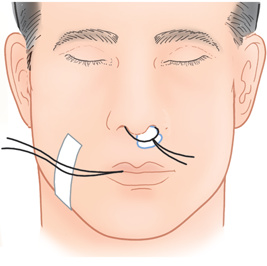
This, but it inserts a little tampon instead of a balloon, and then an attached coiled string at the level of the yellow marker has its end drawn back out the nostril by the insertion tool.
Then the string coming out the nostril is taped to the face, much like this:
Hi everyone
Wow, so many people with PLFs, until I found James on this forum I felt so alone with it, even a professor of ENT (prior to correct diagnosis which took years) told me I categorically didn’t have an ENT issue. It is awful to hear of so many people suffering.
I had my 3rd repair 2 months ago. Caused by a car accident it turns out I had a tear in both right windows AND at the base of the balance part of the ear (the latter causing Tupilo’s syndrome). It’s been a rocky recovery, and I caught a cold 2 weeks ago that sent recovery backwards but it finally appears to be healing. If anyone here has the chance to see Prof Saeed and his entire team at UCLH London (@turnitaround has seen him too) then please go. Don’t bother with local ENT’s, they simply don’t know enough.
Once Prof Saeed’s team fits me with a grommet early next year I will even be able to fly again. I am slowly picking up the pieces of my life after 4 years of all 7 levels of hell, I can’t even begin to tell you. The leak was the largest the surgeons at UCLH had ever seen, I was completely disabled.
But I finally have a light at the end of the tunnel and it is shining brighter every day now, so I hope everyone here finds that too very soon.
Take care all
Tx
Hey guys, before we get carried away completely by the possibility that Perilymph is the fluid, there’s also of course another possibility: Chronic Otitis Media.
Usually I believe this is diagnosed by the doctor visualising your ear drum and identifying if there is any fluid behind it.
It was never brought up as a possibility for me, but then again I wonder if you need a large enough amount of fluid for it to show up on the ear drum. My fluid seems to drain away in seconds when getting out of bed. I’ve also never had an abnormal pressure test. However you do wonder if some issues are too subtle to be picked up on regular tests. Sometimes one detects things which the doctors simply cannot reflect on the graphs.
This sensation has been decreasing in perceived liquid ‘volume’ for 3.5 years for me so it felt like things were ‘healing’ (used to be glug glug, then drip drip, now bubble bubble), so i’ve never pushed for a surgical inspection.
However, it’s worth noting, this ‘fluid’ seems to stick in my eustachian tube sometimes and it can ‘crack free’ sometimes when I open my jaw wide (e.g. whilst eating). This adds credence to it being a mucus like the fluid you get from your nose, which also dries and cracks in exactly the same way (sorry to be so descriptive!).
I recently had a cold and this sensation ramped up … which made me think about the whole mucus theory again.
Given some of us have trauma injuries which may have impacted the ear, it is also possible that there is some inflammation in the middle ear which is causing it to create more mucus.
There has been a study which claims that middle ear upset can cause issues with perilymph production and this might lead to significant impact on the inner ear pressure and in turn more symptoms.
https://www.mvertigo.org/t/vertigo-due-to-eustachian-tube-dysfunction/15932?u=turnitaround
I just want to say this thread is massively educating.